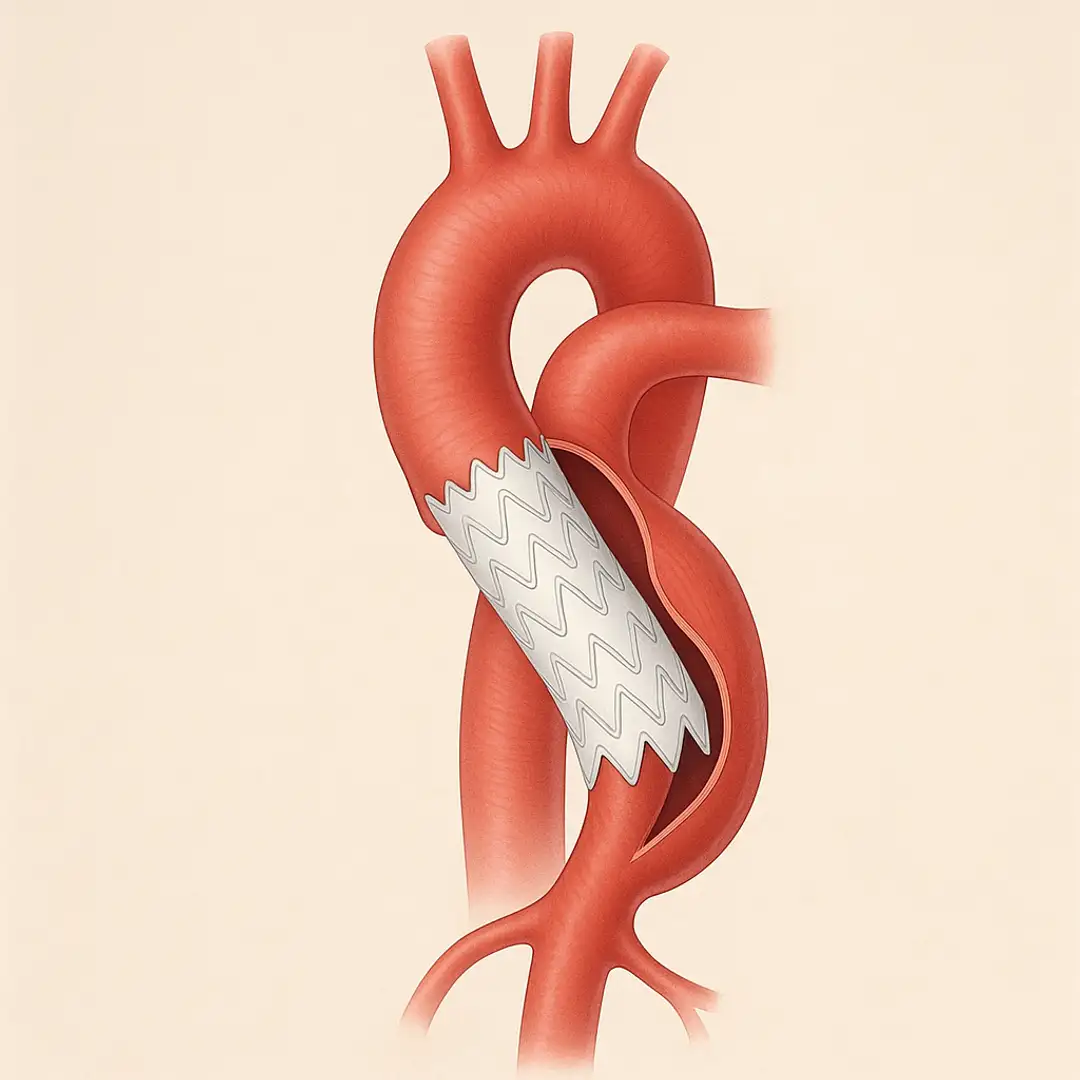
Management of Acute Type B Aortic Dissection.
NEJM review updates practical algorithms: strict medical control for uncomplicated cases, TEVAR for rupture/malperfusion, and lifelong imaging for all patients.

TribeMD
4 min read

September 10, 2025
Sources
- Mussa FF, Kougias P. Management of Acute Type B Aortic Dissection. N Engl J Med. 2025;393(9):895-905. doi:10.1056/NEJMra2405257.
Highlights
SnackableHealth® |Non-cardiac effects in HELIOS-B trial: gastrointestinal symptoms and quality-of-life signals discussed by Drs. Mike Gibson and Tony Urey
In today’s SnackableHealth® episode, Dr. Mike Gibson speaks with Dr. Tony Urey about the idea that amyloidosis can be a multisystem disease—while clinical attention has often centered on cardiac manifestations, particularly in “wild-type transthyretin amyloidosis,” which has historically been framed primarily as a cardiac condition. Dr. Urey explains that, in reviewing the HELIOS B data, the goal was to better characterize under-recognized symptoms that may affect patients’ quality of life. H
ASCO GU® 2026
ASCO GU 2026 (American Society of Clinical Oncology Genitourinary Cancers Symposium) is one of the leading international events dedicated to genitourinary cancers, bringing together specialists from around the world to discuss the latest advances in diagnosis, treatment, and clinical research. Held from February 26 to 28, 2026, at the Moscone Center in San Francisco, California (USA), the symposium is a reference point for the presentation of new scientific data, results fr
Trastuzumab deruxtecan (T-DXd) Provides Significant Clinical Benefit Over Trastuzumab emtansine (T-DM1), Marking a Potential Shift in the Therapeutic Standard for HER2+ Breast Cancer
Breast cancer is the second most common type of cancer and one of the leading causes of cancer-related death worldwide. HER2 is a tyrosine kinase receptor protein with a growth-promoting function, present on the surface of several tumor types, including breast cancer. HER2 protein overexpression, often due to gene amplification, is associated with more aggressive disease and poorer prognosis. Approximately one in five cases of breast cancer is classified as HER2-posit